Gastric Ulcers
Article by Richard Hepburn MS(Hons) CertEM(IntMed) DipACVIM MRCVS
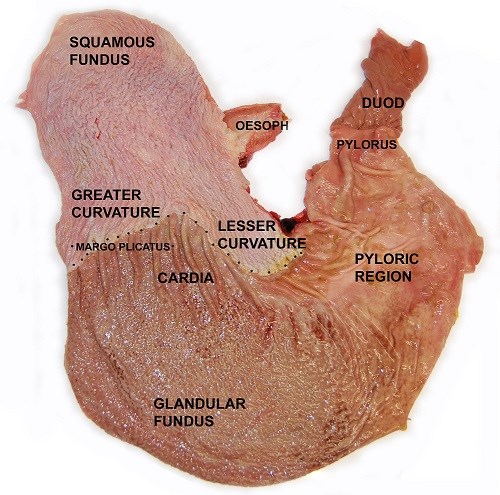
The horse's stomach is covered by two lining tissues: squamous and glandular mucosae: 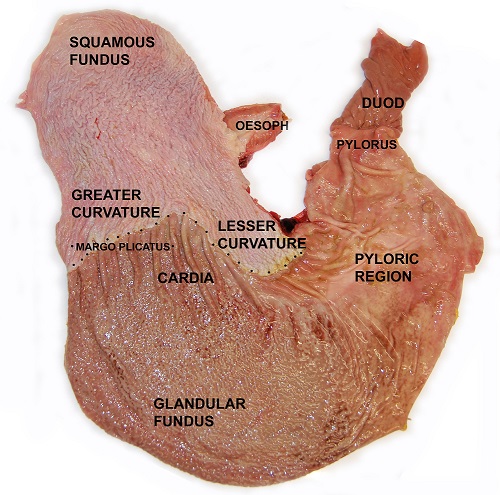
Bleeding from equine gastric ulcers is not a common or consistent finding, so faecal blood/albumin testing is not recommended. The test is also unable to distinguish between squamous and glandular disease, and so targeted treatment is not possible. A better screening approach is to look for significant clinical signs developing in your horse: appetite change, slowed eating, below expected performance and potentially development of behavioural change or resentment of girthing. If these are found then the most accurate diagnostic test is gastroscopy (video-endoscopy of the stomach).
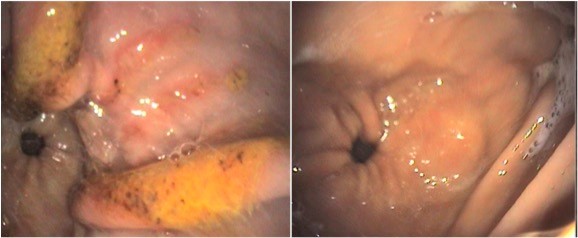
Squamous ulcers affect the white top third of the stomach, and reflect increased acid exposure of the tissue. Their correct name is Equine squamous gastric disease. Ulcers form quickly, and are consistently associated with changes in appetite, slowed eating and poor performance. Inconsistent changes in behaviour/attitude can also occur. Squamous ulcers occur with daytime forage deprivation, lack of access to water, high starch diets, pelleted feeds, straw feeding, intense exercise, change in housing, transport, and lack of daily horse-horse contact. Treatment with an equine formulation of the acid suppressant drug omeprazole is consistently very effective, with the majority of lesions healing within 21-28 days. The image below shows squamous ulcers (left) and the same area healed after 28 days of treatment (right).

Glandular ulcers affect the pink bottom 2/3 of the stomach, in particular the final 1/3 called the antrum. Their correct name is Equine Glandular Gastric Disease. Ulcers form slowly and reflect failure of the mucus coat that protects glandular tissue from acid. The clinical signs are more variable, and may or may not include appetite change/weight loss. In some horses development of resentment to girthing may occur, but this is not specific. The mechanism of failure of the mucus coat is unknown, but could be physical (coarse alfalfa), toxic (drugs or plants), bacterial or physiological (altered mucus constituents). It is likely that several different causes contribute to this failure. Treatment with omeprazole alone is much less effective than in squamous disease (25% healed after 28-35 days); instead a combination of omeprazole and the mucosal protectant sucralfate is used, leading to a 68% healing rate.
In adult horses there is no evidence of a cause and effect relationship between the presence of either type of stomach ulcers and changes in the consistency of their droppings. Diarrhoea is only really associated with gastric ulcers in foals.
In racehorses squamous ulceration can reduce stride length, limit training progression and reduce the time to fatigue; potentially as a result of low grade pain affecting abdominal strength and mechanics of breathing. Similarly treatment studies have shown improved performance measures after ulcer resolution in racehorses. In sport horses we see the same effect of fatigue in eventers. In addition we see cases in all disciplines that show resistance when collecting or extending their stride, or who refuse to jump with ulceration. The evidence for more specific signs such as sensitivity in a certain part of the abdomen, spooking or behavioural change, is anecdotal. If ulcers in an individual horse are suspected to be causing these then clinical improvement should occur as the ulcers heal, and so a critical appraisal of the value of treatment at repeat gastroscopy is essential.
There is also a population of horses that appear normal, but whom benefit from diagnosis and treatment of ulceration. At the same time there are horses that have the same ulcers, which show no clinical signs and no benefit from treatment. Unfortunately it is not possible to distinguish these cases by endoscopy alone, and so a period of test treatment with omeprazole is used to assess their ulcer relevance.
There are two stages to effective treatment of ulcers:
Stage 1
The most effective way to resolve squamous ulcers is with an equine specific form of omeprazole, given at an appropriate dose, for a period of time appropriate for your horse's ulcers: widespread shallow squamous lesions heal faster (14-21 days) than more focal deep lesions (28 days). For glandular ulcers a combination of omeprazole and the mucosal protectant Sucralfate is used, with anticipated treatment duration of 28-56 days. In both cases it is important to make subtle changes to feeding (daytime forage bias, multiple forage sources in the stable, pre-exercise chaff feeding, feeding a coarse mix with grain and chaff, and the addition of corn oil); and management (box and stable mirrors, daily direct horse to horse contact).
Stage 2
Complete healing occurs in over 80% squamous cases, ideally gastroscopy should be repeated but if an excellent clinical response has occurred then this can be skipped and the horse put onto maintenance treatment for a period of 2-3 months. Just stopping at this point is associated with a high ulcer recurrence rate (approximately 80% within 6 weeks).
For squamous lesions there are two maintenance options: firstly continue using equine specific omeprazole but reduce to ¼ dose. This is very effective, and user friendly as it is a once a day treatment. The second option is to use an acid neutralising feed supplement (containing aluminium hydroxide, magnesium hydroxide and calcium carbonate - think 'Rennies' for your horse). This approach is less consistent, and the supplement must be given 3-4 times daily, as its effect is short lived. With either option it is vital that protective feeding and management changes are continued.
In cases of glandular ulceration complete healing occurs in about 70% cases, however some cases actually get worse endoscopically and so repeat gastroscopy is more important. If lesions have healed then the omeprazole dose is reduced over a 6 week period whilst a coating agent supplement is started. Again diet and management changes are continued long term. In both types of ulceration I recommend repeating the gastroscopy after 1-3 months of being on the feed supplement alone, if the horse is happy and the stomach looks good then you have a long term plan. This can be supplemented with a ¼ dose omeprazole when you stay away to compete (start 48h pre-departure, stop upon return home), don't use more than a ¼ dose as it is unnecessary in most horses.
This 2-stage plan has worked in thousands of horses at B&W over the last 15 years (we gastroscope about 350-400 horses per year!). There are a variety of other supplements containing different fibres or proteins, seaweed, plant or mineral extracts, however none of them has been shown to be clinically effective in either the treatment or prevention of either type of ulceration.
The following is the current best advice on feeding to prevent gastric ulceration:
- Allow access to high quality forage, predominantly during the day (7am to 11pm), at a minimum daily rate of 1.5kg/100kg body weight (BWT), ideally given continuously or at no more than 6 hour intervals.
- Multiple forage sources in the stable improve eating consistency and allow foraging activity.
- There is no difference between hay (dry, soaked or steamed) and haylage as a forage source in relation to ulceration.
- Straw feeding should not exceed 0.25kg/100kgBWT, and it should not be the only forage source.
- Free access to fresh water 24 hours a day.
- Concentrate ration should be split into 3, rather than 2 meals per day
- Total starch intake should not exceed 2g per kg bodyweight per day
- Whilst there is no evidence to support the use of specific 'gastric healthy' commercial diets, the use of BETA EGUS approved feeds does ensure that you will not exceed the maximum starch level.
- Chaff should be added to all meals.
- Corn oil or rapeseed oil (50-100ml 1-2 times per day) can reduce the amount of stomach acid produced and could increase barrier mucus function in the glandular mucosa
- Pre-exercise chaff feeding - 2L un-molassed chaff given within 30 mins of exercise may trap acid and limit ulceration, and improve gastric blood supply.